

Preventing arrhythmias and sodium cardiac death through late sodium current inhibition
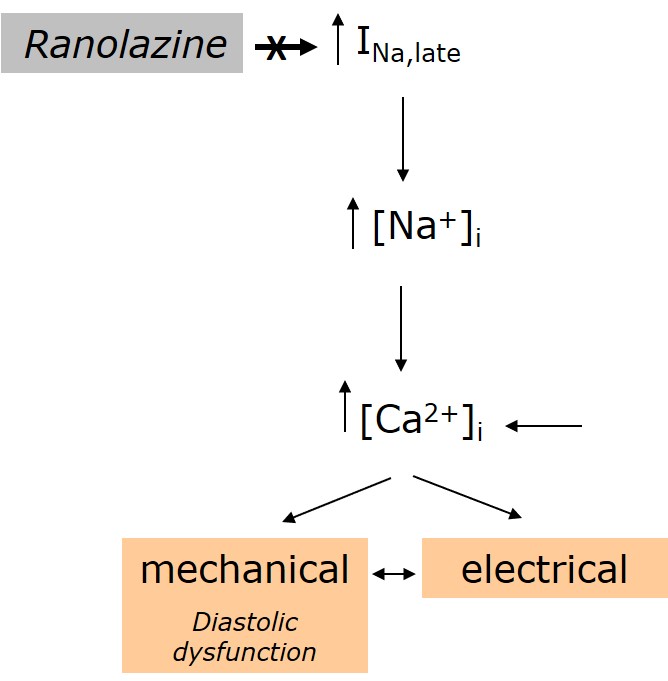
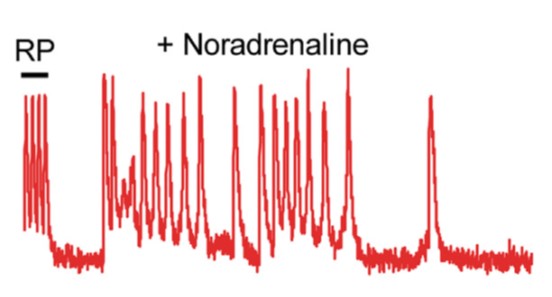
The initial large inward sodium current (peak sodium current) is for the most part rapidly inactivated, but a small fraction of the current (designated the persistent or late sodium current) persists throughout the duration of the action potential (AP) plateau phase. This late sodium current is typically small during physiological conditions, but may be enhanced in the setting of acquired (ischemia, hypertrophy and heart failure) and inherited (LQT3) disease. Independent of the underlying cause, delayed repolarization and action potential prolongation occurs, and early after-depolarizations may subsequently trigger torsades de pointes arrhythmias and sudden death. We have moreover demonstrated that enhanced late sodium current secondary to an SCN5A mutation alters intracellular sodium and calcium homeostasis, further predisposing to arrhythmias (Rivaud et al. Int J Cardiol 2018). Hence, pharmacological inhibition of enhanced late sodium current is an attractive therapeutic target.
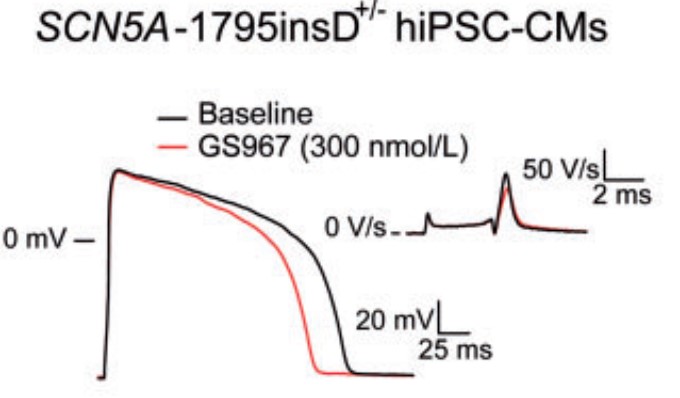
While most agents with general sodium channel blocking effects also reduce late sodium current, the inhibiting effects of these agents on peak sodium current may set the stage for conduction slowing and ventricular arrhythmias, in particular during conditions where sodium channel function is already compromised (i.e. myocardial ischemia). Furthermore, these “classical” sodium channel inhibitors may also impact on other ion channels, in particular potassium channels, potentially limiting their clinical applicability. The more specific late sodium current inhibitor ranolazine may be up to 30- to 40-fold more potent in inhibiting late compared to peak sodium current, and we have shown beneficial effects of ranolazine on late sodium current induced pro-arrhythmic calcium dysregulation, action potential prolongation, AV-conduction and sudden cardiac death (Rivaud et al. Int J Cardiol 2018; Rivaud et al. Eur Heart J 2018). However, its potency varies between species, cell type, and conditions and ranolazine also inhibits the repolarizing potassium current. Recently, a novel highly selective inhibitor of late sodium current, GS-458967 was identified. We have demonstrated beneficial (anti-arrhythmic) effects of this compound in Scn5a-1798insD/+ cardiomyocytes and human iPS-derived cardiomyocytes from a patient carrying the SCN5A-1795insD mutation (Portero et al. Cardiovasc Res 2017).
Our current research is aimed at further exploring mechanisms underlying enhanced late sodium current, in order to facilitate further development of this therapeutic approach towards potential clinical applicability.
Group members
Carol Ann Remme
Group Leader, PI
Vincent Portero
Post Doc
Simona Casini
Post Doc
Giovanna Nasilli
PhD Student
Gerard Marchal
PhD Student